HERETICAL NUTRITION,
MEDICINE, CONSPIRACIES etc
Stan Bleszynski (Heretic) Resume
Updated 28-Feb-2008

Optimal
Line article
Low
Carb (in) Digest
LowCarb(in)Digest#2
LowCarb(in)Digest#3(22-Jan2007)
Links
and References
Seminar 1 (March
2003)
Seminar 2 (April
2004)
Insulin Model (June 2004)
#Human
Metabolism
#Stout
#Eckel
Note: documents and links are presented
here in sections that were assembled mostly in chronological order (if
there is any order at all) to serve as the reference rather than forming
a homogenous essay. The readers (if there are any) are enouraged
to begin with the Low Carb Indigest links to familiarise themselves with
the available research and studies.
Stan B.
NEW
A study
shows that the difference between whole grain and refined grain diets
is statistically insignificant and trends mostly (see Table 1) in favor
of refined grains, against the whole grains.
Four Nutrition Cases
and Diabetes
An overview article compiled by Heretic,
based on Dr.J.Kwasniewski's "Optimal Diet"**
4-Aug-2006
Many if not most doctors seem to be
recommending the low carb diets for their diabetic (t2) patients while
the American Diabetes Assoc. and other medical organizations haven't
yet come to grips with that. It may seem curious that some
official mainstream diabetic and medical organisations recommend to eat
50-60% carbs while at the same times the doctors are telling patients quietly
to go Southbeach or Atkins. Naturally medical doctors or nurses
cannot acknowledge that their recommendations are in conflict because they
stand to loose if they suddenly challenged their own institutions.
It is important to stress then fact
that most doctors are not yet aware of the existence of a dangerous medium
carb medium fat zone when one tries reducing carbs but not quite enough
and increasing fat intake, but not suffiently so.
When one reduce carbohydrates to about
~30-40% and increasing fats to ~35-45% calories**, it may in fact
result in the worsening of the diabetes symptoms for diabetics, and in
the increased risk of getting diabetes for healthy people, especially middle-aged
adults and elderly. In that intermediate zone the amount of fat becomes
high enough that body metabolism switches over to "burning" fatty acids
and ketone bodies (our bodies prefer using fat and ketones for energy,
over carbs). However when metabolism switches over towards fats it increases
at the same time the insulin resistance factor, in order to block the insulin
transport into the tissue cells. That insulin blokade serves the
purpose of slowing down or blocking the glucose catabolic (="burning")
pathways inside the cells, since both fat and glucose metabolic channels
do not seem to coexist very well simultanously at the cellullar level.
Yet the amount of carbohydrates consumed in this intermediate zone is still
hight enough to cause the excessive and unwanted blood glucose to circulate
in the bloodstream that still has to be somehow dealt with otherwise it
would raise the concentration to a dangerously high level.
Since the glucose catabolism is slowed down by the insulin resistance factor,
body has no choice but to keep increasing the insulin concentration (by
pancreas) to overcome the resistance until blood glucose level is brought
back under control. In case of diabetes this additional insulin may
have to be injected.
To simplify things, I one can identify
the four distinct dietary zones:
1) low fat (below 30%)
high carb (above 40%), low caloric zone (below about 25 kcal/kg/day*):
Body has no choice but to use all the
carbohydrates for energy thus insulin resistance is low but blood insulin
level is medium (cannot be very low since it is required for metabolism
of glucose sugar).
Diabetes type 2 symptoms partially reverse
but do not disappear completely.
2) low fat (below 30%)
high carb (above 40%), high caloric (above 35kcal/kg/day):
Body receives excessive carbs and deals
with the excess by converting part of carbohydrates (especially fructose!)
into fat (triglycerides!). Insulin resistance increases and blood insulin
level is high.
Note: the negative effects in this zone
are exacerbated in the high carbohydrate limit (towards and beyond 60%)
if the protein intake is too low, for example if the carbohydrate contents
is above 60% and if the protein contents is below 20% (or less than about
2g/kg/day) then the amount of aminoacids available for enzyme production
may be insufficient to efficiently digest and metabolize all carbohydrates.
In that case body has no choice but slow down the activity and convert
the increasing percentage of carbohydrates into fat rather than using it
for energy. Another factor that may push metabolism towards converting
carbs into fat for storage as opposed to "burning", is magnesium and zink
defficiency, oxygen defficiency, excess of calcium, or overactivity of
parasympathetic autonomous nervous system.
Diabetes type 2 symptoms tend to get
progressively worse over time.
3) Medium fat (35-45%
calories) medium carbohydrates:
Body switches to fat metabolism and
insulin resistance becomes very high. Blood insulin level is the highest
(or is required
to be very high to maintain normal
blood glucose level).
In diabetes type 2 this is the worse
condition to be in. For healthy people this is the most obese-inducing,
the most diabetes-inducing and the most arteriosclerotic diet. A
case when such a diet may be benefitial (for a short time!) is deep free
diving sport since it reduces the body oxygen requirement.
4) Very high fat, very
low carb (less than 1g/kg/day) and medium protein (1-1.5g/kg/day):
Insulin resistance is high due to fat-oriented
metabolism but blood insulin level and the insulin requirement is the lowest
due to the very low carbohydrate turnover. Body tissues switch over to
fat and ketone metabolism to conserve glucose. Ketone bodies are superior
fuel for brain, neural tissue (e.g. epileptic diets!) and heart muscle.
Ketone metabolism seems also to suppress cancerous growth. It seems to
be our bodies' most natural type of metabolism.
In diabetes type 2: most symptoms reverse
very quickly and completely, within typically 2 weeks to a couple of months.
Stan Bleszynski
-------------------
Footnotes:
*) the numbers given as "X something
per kg/day" mean that X has to be multiplied by the ideal (not actual)
body weight in kg in order to obtain the daily dose.
**) J.Kwasniewski, M.Chylinski
"Homo Optimus" and "Optimal Nutrition"
http://www.cybernaut.com.au/optimal_nutrition/books.html
http://www.wgp.com.pl/index.php?id_s=205&id_j=en
http://homodiet.netfirms.com/
Recommended book:
"Body Mind and Sugar"
Author: Abrahamson, E.M. & Pezet, A.W.
Publisher Henry Holt, New York, 1959
NEWImportant
research study, The Lancet, 1968,1969:
Two experiments on rats
using isotope carbon-14 tagged molecules, by R.W. Stout, demonstrating
that arterial deposits probably come out of blood glucose in presence of
insulin, and are unlikely to come from dietary cholesterol!
Download
paper 1 (pdf, 200k)
Download
paper 2 (pdf, 200k)
Treatment of Viral Diseases
Subject:
SP Re: West Nile
Date: Fri,
06 Aug 2004 11:17:06 -0400
From:
Stan Bleszynski <stanb@ptbo.igs.net>
To:
Stan P. [...]
Stan P. wrote:
Severe
complications of West Nile virus, such as inflammation of the brain or
nerves, have affected 156 patients, or about 38 percent of reported
cases, CDC said. Only 29 percent of patients had such complications
last year, according to the CDC Web site. This is strange. Official risk
assessment states 20% infected get fever, but only 1 in 150
gets encephalitis or meningitisSo is it less then 1% or 38%? Any idea why
infection rate is
growing?
I have a hypothesis:
the difference may have reflected the fact whether the patients were treated
in hospitals with standard anti-viral drugs (38% complications) versus
left at home (1%).
This occured to me last year when watching
SARS unfolding slowly and then mysteriously disappearing suddenly
in May 2003.
* - The disappearance of SARS in
Toronto coincided with the closure of hospitals.
** - I have seen specific data from Singapore
(private communication) when up until end of April there were 200 patients
in the hospital, at the time when the health minister issued administrative
directive banning the use of existing drug treatment. That happened
on the 23'rd of April. Afterwards every single one of those
200 patients fully recovered within 2 weeks - there was zero mortality!
*** - Striking discrepancy between SARS
mortality rates among ethnically similar populations in Hong Kong (5%),
in the mainland China (about 1-5%), in the USA (about 1-5%) and Toronto
(10%) indicates a presence of some artificial factor unrelated to the disease
itself. Such a factor may be a different rate and the type
of drug treatment. For example in Toronto everybody was treated since
the "health" system is "free". In the US, HK and mainland China
the health coverage was only partial (in China people were avoiding reporting
to hospitals because of a risk ivolved with the police procedure and heavily
handed quaranteen).
**** - side effects of antibiotics, another
commonly used "treatment" for flu and SARS (at that time) is a suppression
of body's unspecific immune system, that's why patients become more susceptible
(by 40% on average) to further infections, following a discontinuation
of the drug. Especially they become prone to fungal (yeast) infections
since these are not affected by the antibiotic itself.
The suppression of the immune system manifests itself by an almost immediate
reduction in fever and inflammation which most medical "professionals"
mistakenly take as a positive symptom. It is far from being
positive because it slows down the healing and it allows the virus to hide
in some tissues, become dormant for some time, to acquire enough
time mutate/evolve to become less detectable by the leukocites. This
process may allow a relatively benign flu (=mortality rate of the order
of 1/1000) to turn into a much worse disease such as "chronic fatigue"
(=probably in nerves or in spinal cord), meningitis (brain) or cardiomyopathy
(heart muscle disease) or valve damage.
**** - Ribavirin (standard anti-viral drug
for respiratory illnesses) works by interfering with the viral RNA replication
mechanism, inducing rapit mutations[1]. This seems to
induce side effects that look to me like that it interferes also with the
normal body's energy producing mechanism in the cells (this is my speculation
SB) which affects general energy level, and have particularly strong impact
on energy hungry organs such as heart muscle and brain, see [2].
Interestingly these side effects are virtually identical to those listed
for statin drugs which is another class of drugs that interfere with the
body energy conversion channels. As such it may not only compromise
body's ability to heal itself, but it may also increase the natural speed
of mutation that may conceivably make some population of benign viruses
that survive the treatment - more lethal.
...
---------
Fotnotes -----------------------------------------------------------------
1) RIBAVIRIN
MECHANISM
http://www.aidsmeds.com/news/20010521drgd009.html
WESTPORT,
CT (Reuters Health) - The antiviral agent ribavirin has been shown to work
by inducing genetic error catastrophe in RNA viruses. "Hopefully, the discovery
of ribavirin's mechanism of action, which had been a mystery for 25 years,
will lead to new drugs, related to ribavirin, that are useful against many
different types of RNA viral ailments," lead investigator Dr. Raul Andino
told Reuters Health. "This is quite exciting."
Dr. Andino,
of the University of California, San Francisco, and colleagues report their
discovery in May 22nd online Early Edition of Proceedings of the National
Academy of Sciences.
In December,
the same research team published findings in Nature Medicine (see Reuters
Health report, December 12, 2000) demonstrating that ribavirin is an RNA
virus mutagen, and they proposed that lethal mutagenesis was ribavirin's
mechanism of action.. "However, in that preliminary study, we were only
able to show a correlation between ribavirin's mutagenesis and the antiviral
effect," Dr. Andino said.
The PNAS
paper "directly proves that lethal mutagenesis is ribavirin's mechanism
of action." He said that it's the first time that lethal mutagenesis has
been proven as an effective antiviral drug strategy.
RNA viruses,
like those for HIV and influenza, have a naturally high mutation rate,
Dr. Andino explained. Ribavirin overwhelms these viruses with a flood of
mutations, sending them into error catastrophe. This is "surprising because
it seems counterintuitive," Dr. Andino said. "It would seem that a high
mutation rate would help the virus escape the drug. But, that's not the
case."
Using
poliovirus, the team observed a 99.3% loss in viral genome infectivity
after a single round of ribavirin mutagenesis sufficient to cause a 9.7-fold
increase in mutation frequency.
"This
discovery provides pharmaceutical companies with a good RNA virus drug
target (the RNA-dependent RNA polymerase enzyme), a whole new drug development
strategy (RNA virus mutagens), and a compelling example (ribavirin) that
this strategy can actually work," Dr. Andino said.WESTPORT, CT (Reuters
Health) - The antiviral agent ribavirin has been shown to work by inducing
genetic error catastrophe in RNA viruses. "Hopefully, the discovery of
ribavirin's mechanism of action, which had been a mystery for 25 years,
will lead to new drugs, related to ribavirin, that are useful against many
different types of RNA viral ailments," lead investigator Dr. Raul Andino
told Reuters Health. "This is quite exciting."
Dr. Andino,
of the University of California, San Francisco, and colleagues report their
discovery in May 22nd online Early Edition of Proceedings of the National
Academy of Sciences.
In December,
the same research team published findings in Nature Medicine (see Reuters
Health report, December 12, 2000) demonstrating that ribavirin is an RNA
virus mutagen, and they proposed that lethal mutagenesis was ribavirin's
mechanism of action.. "However, in that preliminary study, we were only
able to show a correlation between ribavirin's mutagenesis and the antiviral
effect," Dr. Andino said.
The PNAS
paper "directly proves that lethal mutagenesis is ribavirin's mechanism
of action." He said that it's the first time that lethal mutagenesis has
been proven as an effective antiviral drug strategy.
RNA viruses,
like those for HIV and influenza, have a naturally high mutation rate,
Dr. Andino explained. Ribavirin overwhelms these viruses with a flood of
mutations, sending them into error catastrophe. This is "surprising because
it seems counterintuitive," Dr. Andino said. "It would seem that a high
mutation rate would help the virus escape the drug. But, that's not the
case."
Using
poliovirus, the team observed a 99.3% loss in viral genome infectivity
after a single round of ribavirin mutagenesis sufficient to cause a 9.7-fold
increase in mutation frequency.
"This
discovery provides pharmaceutical companies with a good RNA virus drug
target (the RNA-dependent RNA polymerase enzyme), a whole new drug development
strategy (RNA virus mutagens), and a compelling example (ribavirin) that
this strategy can actually work," Dr. Andino said.
2)
RIBAVIRIN SIDE EFFECTS
http://www.nlm.nih.gov/medlineplus/druginfo/uspdi/202509.html#SXX
Quote:
...
Ribavirin
for oral use should not be used while you are pregnant, if you plan on
becoming pregnant, or by men whose female partners are pregnant or are
planning to become pregnant. It has been shown to cause serious birth defects
and other problems in animals. Be sure you have discussed this with your
doctor.
...
A negative
pregnancy test is needed in women who are of childbearing age before starting
treatment with oral ribavirin. Two forms of birth control must be used
during oral ribavirin treatment and for six months after treatment ends.
...
Chest
pain; difficult or labored breathing ; pale skin; shortness
of breath; tightness in chest; troubled breathing with exertion;
unusual bleeding or bruising; unusual tiredness or weakness;
wheezing
...
More
common
Acid
or sour stomach; belching; discouragement; dizziness;
feeling sad or empty; feeling unusually cold; heartburn;
indigestion ; irritability; itching skin; lack of appetite;
loss of interest or pleasure; lack or loss of strength ; shivering;
stomach discomfort, upset, or pain; tiredness; trouble concentrating;
trouble sleeping
Less common
Change
in taste; cough; crying; depersonalization; difficulty
in moving; dysphoria; euphoria; fatigue; fever;
gastrointestinal effects; headache; insomnia; joint pain;
mental depression; muscle aching or cramping; muscle pains
or stiffness ; nervousness; pain or tenderness around eyes
and cheekbones; paranoia; quick to react or overreact emotionally;
rapidly changing moods; rash; shortness of breath; stuffy
or runny nose; swollen joints; vomiting
Rare
Itching,
redness, or swelling of eyes; skin rash or irritation
A
Case For High Fat Nutrition
Based on the presentation
by Dr. R.H.Eckel, spokesman for the American Heart Assoc., The 25th Lillian
Fountain Smith Conference for Nutrition Educators, Fort Collins Marriott,
June 5-6, 2003
(re-edited 6-Aug-2004)
http://www.cahs.colostate.edu/fshn/lfsc/Nutrigenomics.pdf
What is really interesting is data and
graphs. Let me summarize what I found the most exciting:
1) Graph on page 3 "Cumulative Distribution
of Adjusted Plasma TG Levels: LDL Phenotypes A and B"
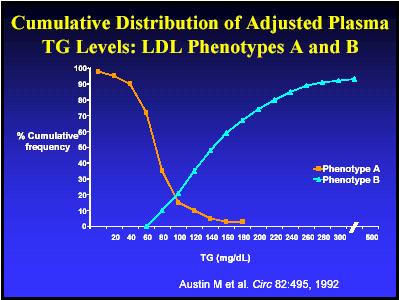
It shows that above the triglycerides level
of 100mg/dl, LDL phenotype B (the one that is "Associated with pro-atherogenic
metabolism") dominates!
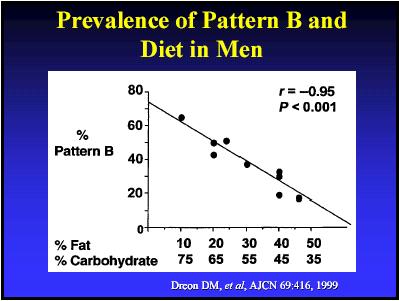
2) Graphs on page 3 and 4 titled:
"Distribution of Changes in LDL
Cholesterol in Men with Diets of
24% vs 45% Fat" and "Prevalence of
Pattern B and Diet in Men"
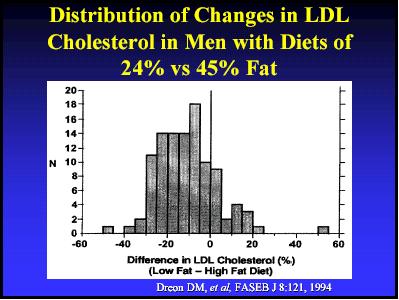
The first graph shows that men who ate
45% fat had about 115% (range 80-130%) LDL cholesterol level as compared
with those who ate 24% fat (=100% relative LDL level) .
However the second graph (LDL-B versus dietary fat) shows that at the same
time those who ate 45% fat had only 20% of that cholesterol in phenotype
B while those who ate 24% had 50% of LDL-B! In other
words, those who ate 45% of fat had SLIGHTLY higher total LDL but had MUCH
lower level of the dangerous LDL phenotype B fraction, then those who ate
24% fat! The second graph (Dreon DM,et al, AJCN 69:416, 1999)
shows also that at above the dietary fat contents of 60% (Atkins diet!)
and below dietary carbohydrates contents of 25%, the LDL-B becomes ZERO...
3) Slide on page 4 titled "HDL"
- shows that the so-called "good cholesterol"
HDL is inversely related to Coronary Heart Disease (CHD), decreases with
dietary carbohydrates (abbrev. "CHO" on the graphs) and increases with
dietary fat!
Slide on page 4 titled "HDL and diet"
- shows that HDL increases with increased
saturated and monounsaturated dietary fats, and decreases with polyunsaturated
fats and carbohydrates (CHO). Drawing a logical conclusion, it follows
that Coronary Heart Disease should INVERSELY correlate with dietary saturated
and mono-unsaturated fats, and POSITIVELY correlate with polyunsaturated
fats! In other words, according to
the presentation, consumming more saturated and monousaturated fats ought
to reduce the rate of coronary heart disease which is exactly the opposite
to the message AHA and other organisations are officially propagating to
the public! By the same token, diets high in carbohydrates
and polyunsaturated (vegetable mostly) fats ought to be increasing a risk
of coronary heart disease, contrary again to the message propagated officially
by most medical organisations!
4) Slides on page 6 titled "Type 1 Diabetes"
- present an interesting theory ( Amanda
J.MacFarlane et al, J.Biological Chem.,278,Jan 2003 ) on the possible
link between diabetes type 1 and wheat protein sensitivity.
The paper states that unusual sensitivity to low molecular mass wheat proteins
was observed in humans and in diabetic rats (type 1).
So much for the cereals and whole grain bread that is being touted by most
medical organisation and commercial interests as being a "healthier" alternative
to refined flour products.
Hypertension
http://boards.health.msn.com/message.asp?message_id=4937115
Re: High Sugar and BP related?
by DrBNazario, on 9/24/2003 5:41:27
PM
Sounds like you may have diabetes. Are
they related? Yes on many levels. Diabetes, especially type 2 diabetes,
results from excess amounts of insulin that does not seem to work well
in the body,, the body actually is quite resistant to insulin that is present.
The excess insulin, at first, may be able to normalize blood sugars but
over time it becomes less efficient in dropping sugars to normal ranges.
This excess insulin does cause harm, even prior to high blood sugars, people
with what is known as prediabetes do have a higher than normal risk of
heart disease and heart related problems like high blood pressure.
Insulin causes vessels to dilate or relax. The excess insulin that really
doesn't function as well as in non diabetic people is also not sense by
blood vessel-- like arteries. Relaxed vessel means non-stiff vessel. When
the heart pumps blood into the vessels they shouldn't act like stiff pipes.
People with high blood pressure have stiffen arteries . People with diabetes
have stiff vessels possible caused by the fact that they cannot relax their
arteries because insulin doesn't function normally in them and the arteries
do not relax.
If you have high blood pressure it is
important that you do the things that you should to lower the levels to
130/80. Lifestyle changes like exericse, weight loss, discontinuing tobacco
use, decreasing salt consumption and fat intake will all help . Your doctor
may put you on blood pressure pill. You may not at all feel any different.
Remember that high blood pressure is a silent killer. It will slowly over
time destroy your kidneys, memory, eyes,increase your risk of stroke and
heart attacks...
Re: Re: Re: High Sugar and BP related?
by Heretic, on 9/26/2003 9:22:29 AM
Re: "While the data is preliminary, it's
supportive of MDs aggressively treating BP to not only 130/80 but to 115/75
especially in patients who adjust easily to RX therapies?"
Possibly, but there may also be a counter-indication.
Hypertension medications seem to act by stimulation of the parasympatetic
autonomous nervous system. The side effect of which is acceleration of
the formation of arterial plaque which forms particularily rapidly under
metabolic "pentose shunt" channel which seems to be controlled by the parasympatetic
system.
According to dr. Kwasniewski's "Homo Optimus",
overactive parasympatetic nervous system promotes glucose and fat metabolism
thrugh the so-called "pentose shunt", which is also favored by the conjuction
of the following three factors:
1) high glucose supply
2) high insulin supply
3) high lipoproteins & triglycerides
supply
That condition is also brought about by
fat and carbohydrates consmed in comparable proportions.
I find dr. Nazario explanation on the action
of excessive insulin on BP very interesting, and it may in fact be giving
us the clue on the most efficient treatment of BP, alternative to the direct
blood pressure medications (beta blockers, calcium channel blockers, diuretics
etc). Namely, if excessive insulin is the primary cause of the arterial
insensitivity, then the treatment which resulted in lowering of the insulin
level should also remove the primary cause of BP!
Since insulin is secreted directly in response
to consumed carbohydrates (and to some smaller extent, proteins) then reduction
in carbohydrate consumption should automatically reduce blood insulin levels,
which then should alleviate insulin resistance factor (IR develops in response
to excessive insulin), which should then result in reduced blood pressure.
In addition, since pure carbohydrate metabolism uses up 30% more oxygen,
lower carb consumption might improve the overall tissues oxygenation (especially
brain and heart) almost immediately (I have seen reports indicationg that
hypertension might in fact arise also in response to underoxygenation).
Human
Metabolism
Dr. Jan Kwasniewski's
article on metabolism and arteriosclerosis,
Hexose and Pentose glucose
cycles.
(Review by Stan Bleszynski
28-April-2003)
See also
Insulin Model
The following review is posted also on:
http://boards.health.msn.com/message.asp?message_id=3892893
This review is written especially for people
who found that high fat low carb diets work for them but are curious to
know why. There was a very interesting radio-internet transmission
program on Saturday 26-April-2003 with dr. Jan Kwasniewski, emitted by
Wloclawek Radio. Kwasniewski talked about possible explanations of arteriosclerosis
in the context of metabolic processes and nutrition. I have
already mentioned some of the issues in my past posts, however, I thought
it would be useful to recap it again for the sake of people who found that
high fat low carb works, but would like to know why. One should keep
in mind that it is not a complete study, just an article based on
medical practice of one doctor plus his literature research.
Two metabolic pathways of glucose:
1) Hexose cycle.
Glucose is OXIDIZED and about 4
Cal/g is extracted in the catabolic (="burning") process, going through
a very complex reaction chain involving multiple stages where hormones
like insulin and minerals like Magnesium are necessary components.
The problem with hexose cycle is that some but not all body tissues can
thrive or can utilize glucose as fuel efficiently. One such tissue is the
heart muscle which has the highest volume of mitochondria of all, thus
it means that it is by its nature meant to process mostly fats not
glucose mitochondrias are organellas specializing in metabolizing lipids).
When heart muscle is forced to use glucose because of lack of lipids or
ketone bodies, it may grow abnormally large in size, become inefficient
and uses up too much oxygen. Such condition leads to cardiomyopathy. Another
such tissues is skin and arterial walls.
2) Pentose cycle (sometimes refered
as "Pentose Shunt").
Glucose is REDUCED and about 0 kcal/g
or less than 0 (endothermic) is extracted in the metabolic (="transformation")
process, going through a very complex process involving multiple stages
where hormones like insulin and minerals like Magnesium are necessary components.
This oxygen is then utilized to burn fat releasing about 9kcal per 1g of
fat. One of the by-products of the pentose cycle is cholesterol depositing
in the tissue (but not in blood) and triglycerides (produced in liver and
release into bloodstream). Since pentose cycle allows extraction of oxygen
out of glucose, the overall oxygen intake out of air is reduced thus such
process may be advantageous for survival in some temporary situations.
Now the key point of the article was Kwasniewski's
own observation that it is the Pentose, not Hexose glucose cycle that is
associated with arterial plaque formation, diabetes type 2, obesity and
few other characteristic symptoms. He was able to quantitatively correlate
the absolute intensity of the pentose cycle taking place with arterial
plaque formation, and also the ratio between the pentose-to-hexose pathways
to the same. The absolute intensity of the pentose cycle is proportional
to both the total amount of carbohydrates and fats consumed! This, for
the sake of illustration can be modeled symbolically by the formula:
Pentose intensity =
Carbs * Fats * k
The most interesting information is that
the turning point where the pentose cycle is at MAXIMUM is when the amount
of dietary fat is within this narrow range of 35-45% of calories, while
carbohydrates constitute also a similar fraction, by calories!
Note that this is not always as straightforward since there are situations
when despite the equal presence of fat and carbohydrates pentose
cycle my be artificially suppressed. Such situation takes place when there
is overabundant supply of oxygen, especially when the body is very healthy,
cardiovascular and pulmonary systems are efficient (=young people) and/or
when the sympathetic autonomous nervous system is artificially over-activated,
while the parasympathetic is suppressed (parasympathetic promotes pentose
cycle!), and when the total amount of food calories is slightly below the
normal amount or semi-starving (when body cannot afford to under-utilize
carbs calories through pentose cycle).
For mathematically minded like me, one
can say that the proportionality factor k is a function of the above-listed
conditions, that is:
k=f(Para/Symp, total
cal, total oxygenation) , etc.
How to minimize pentose cycle?
A) MINIMIZE FAT
That is, when there is very little fat
then the pentose cycle does not take place and instead, most of the carbohydrates
are metabolised through the first process (hexose cycle). That is possibly
the best explanation behind the partial success of the Ornish's very low
fat diet! Since it has very little fat and low in total calories as well,
there is very little pentose cycle taking place, thus the plaque formation
is stopped. Since such diet, at the same time undernourishes arteries (which
require lipids) it also explains why the process is only stopped but cannot
fully reverse and heal the arteries. Although overactive hexose with suppressed
pentose cycle does stop the plaque formation, it may also bring its own
specific health risks among which is hardening and weakening of the arteries
(but without the plaque!), hypertension, undernourishment of skin and certain
other tissues (e.g. eye cornea), weak immune resistance to infections and
changing of the body tissue protein signatures that may trigger auto-immune
agression reaction which may lead to auto-immune diseases such as asthma,
eczema, MS, diabetes t1, Crohn's etc.
B) MINIMIZE CARBOHYDRATES
Apart from reducing fat, pentose cycle
can also be easily minimized by increasing fat and simultaneously
by reducing carbohydrate consumption down to about 10% of calories
or less! Note that once the pentose cycle intensity goes below a certain
threshold, its toxic long term effects are no longer present while the
beneficial temporary reduction in oxygen requirement may be beneficial.
This is the main metabolic rationale behind the high fat low carb diets
such as Kwasniewski's "Optimal Diet", Atkins' or Lutz, and the reason
for their therapeutic successes.
---
Diabetes type 1 - discussion on theory and mechanisms of origin
http://boards.health.msn.com/forum/message.asp?message_id=3898069
Diabetes: A theory
by Stubby0, on 4/27/2003 0:39:49 PM
I have a theory that when each of us is
born, we are given a specific number of pancreatic beta cells just the
way our eye
color is determined. As we live our lives,
we use up those beta cells and become "diabetic". So, if you believe the
theory, all
of us will become diabetic if we live
long enough. Eating a lot of sugar uses up the beta cells faster.
What's scary is the number of overweight
kids who are chowing down on high-sugar, high-fat food. If I'm right, we
are going
to see a dramatic lowering of the average
age that T2 is discovered. Maybe that has started already.
Comments?
Re: Diabetes: A theory
by Heretic, on 4/28/2003 10:04:00 PM
NEW!
You are probably refering to type 1, since
type 2 is related more to insulin resistance rather then the lack of insulin
?
Your theory is probably incorrect, at
least not in all type 1 cases because some studies have shown that an onset
of diabetes
type 1 is accompanied by the presence
of anti-bodies against the beta cells.
Therefore it would indicate that beta
cells are simply being killed off by bodys' own immune system rather then
their number
running down due to exhaustion.
Also, the beta-cells killing process is
rarely 100% since most t1 diabetics (about 90% cases) do retain about 10%
of their
residual insulin producing capacity, that
is about 10 units a day. It seems that the body is getting rid of what
it considers the
excess insulin production capacity leaving
just barely enough to survive, but only on a very low carb, low protein
diet. This
residual capacity seems to be maintained
indefinitely (based Arkadia sources) and don't seem to be running out of
supply.
However the exhaustion mechanism of your
theory may be partially true, since perhaps the exhaustion due to overproduction
of the insulin due to too much dietary
sugars may be altering the protein structure of beta cells enough to trigger
an
auto-immune attack. Immune system will
normally attack and eliminate cells that are abnormal, weak or dying.
It is all speculative of course.
Heretic
Diabetes type 2 - discussion on theory and mechanisms of origin
http://boards.health.msn.com/forum/message.asp?message_id=3870519
Sugar Doesn't Cause Diabetes in Women
by Kyra_WebMD_Staff, on 4/23/2003 9:37:12
AM NEW!
When it comes to preventing type 2 diabetes,
women don't need to shun sugar. In fact, total calories and a sedentary
lifestyle
play larger roles in putting women at
risk. Excess Calories Increase Type 2 Diabetes Risk -- Especially
If You Don't
Exercise.
http://boards.health.msn.com/forum/target=_blank
Kyra
Re: Sugar Doesn't Cause Diabetes in
Women (it most likely does!)
by Heretic, on 4/23/2003 8:11:14 PM
NEW!
I disagree, yes it does! Not only in woman.
The mechanism works as follows:
1) Too much carbohydrates (sugar and any
kind of simple and complex carbs!)
2) High blood insulin level develops which
is required to metabolize carbohydrates
3) Some body tissues develop insulin resistance
in response to raised insulin level
4) Pancreas produces even more insulin
to overcome insulin resistance, thus blood insulin level rises even higher
5) Very high blood insulin level promotes
expansion of fatty tissue and creates strong cardiovascular risk, promoting
arterial
plaque. Insulin also has immunosuppressing
properties and promotes growth of cancerous cells.
6) Eventually pancreas reaches its maximal
yield and cannot produce enough insulin to overcome rising insulin resistance,
which leads to a relative defficiency
of insulin action.
7) Blood glucose first increases its fluctuations
from too low to too high (hypoglycemia and hyperglycemia), then eventually
the
average level rises leading to diabetic
symptoms (type 2). In some minority of cases immune system develops anti-bodies
to
the insulin producing cells leading to
abrupt cessation of insulin production altogether (and diabetes type 1,
though there may
be other causes for d.t.1).
8) Medical doctor then puts a patient on
insulin resistance reducing drugs, insulin injections (or both) for life,
then tells a
patients to continue eating lots of "heathy"
cereals, vegetables and fruit, all low fat ("heart-healthy") of course
...
Heretic
Diabetes - Atkins diet and glucose versus insulin control
http://boards.health.msn.com/message.asp?message_id=4462324
Atkins Diet
by jo2pat, on 7/24/2003 7:28:32 AM NEW!
I recently did the Atkins diet with putting
myself in real danger. I am 20 pounds overweight but was fine cholesterol
and glucose was fine. While being on Atkins I went from 208 cholesterol
to 275 glucose went from 81 to 110. After 2 months I only lost 1 pound.
Well I went back to my high comlex carbs diets lots of veggies and whole
grain snacks. My cholesterol is now 210 glucose back to 81
jo2pat@mailexcite.com
Re: Atkins Diet
by Heretic, on 7/24/2003 0:16:16 PM
NEW!
Sometimes problems may happen if people
try Atkins with insufficient intake of fats.
It should contain at least 60% of calories
out of natural prefereably saturated and mono-unsaturated fats. If you
are diabetic or pre-diabetic with impaired glucose tolerance or hyperinsulinemia
or insulin resistance, then you should also restrict protein intake as
well, to about 1g/1kg body per day, and up the fat to 70-80% of calories.
Of course there may still be another reason.
However saying so I need to emphasize that glucose level of 110mg/dl is
still perfectly normal! On a high fat low carb diet glucose level is slightly
higher then on a high carb but it is also very steady throughout the day,
whereas on a high carb diet it is slightly lower in average (except in
diabetes) but it is also fluctuating wildly. In fact the real indication
of whether you sugar is normal or not is to take a profile throughout the
day and register the minimum-to-maximum spread. As an example, if yours
is going from 60-140mg/dl then you may have a pre-diabetic problem. On
the other hand, if it is always within 120-140mg/dl throughout a day (on
high fat) - then it is fine!.
Re: cholesterol
This is probably not very relevant in your
case, unless you have other risk factors. Cholesterol by itself is not
a risk factor but rather a second-removed indicator of your liver function
and metabolism or massive tissue repair processes going on inside your
body.
In the abscence of other risk factors you
can probably safely ignore cholesterol whether it is 200 or 270mg/dl. Mind
you, for people with very low level, like below 150mg/dl their CVD risk
indeed may be much lower but their cancer risk is instead much higher (see
Framingham study). On top of that there is absolutely no proof that if
you lower your cholesterol by drug or diet to below 150, that it would
have had the same effect as if your cholesterol was so low naturally, by
genetics.
Correlation between cholesterol level and
CVD or any other diseases is very weak indeed. See Uffe Ravnskov book "The
Cholesterol Myth" and all the major government sposored population research
studies (but not the media press releases!) - are supporting this conclusion.
Heretic
Re: Re: Atkins Diet (I should also add...)
by Heretic, on 7/24/2003 0:25:11 PM
NEW!
... that you may perhaps be putting yourself
on higher risk by going back to high carbohydrate nutrition. Cholesterol
notwidthstanding.
Heretic
Re: Re: Atkins Diet
by bill7b, on 7/24/2003 0:38:27 PM
NEW!
I'm not a doctor. I'm a diabetic who was
diagnosed 25 years ago.
In my non-medical opinion, you are way
off-base about glucose levels. A glucose level of 120 to 140 is definitely
not acceptable, for anyone. A blood glucose level that hovers around 110
during the day, all day, isn't ok either.
Bill
Re: Re: Re: Atkins Diet
by Heretic, on 7/24/2003 3:17:47 PM
NEW!
Bill,
Then your opinion contradicts the official
medical guidelines as of up until last year or so. The threshold for diagnosing
diabetes was 140mg/dl, not 110. It has changed recently (I don't know what
it it now). Also, body impulse response (in engineering terminology) after
drinking 50g of glucose is measured to determine whether a patient is diabetic
or not. Not a single reading, even if it is 140. Bottom line is:
- stable reading not fluctuating = no diabetes.
and
- unstable reading fluctuating ABOVE and/or
BELOW the limits (I think it is 60 and 140 but I am not exactly sure of
the numbers, it could be 70 and 130 etc) = diabetes!
Based on the above criteria, 110mg/dl is
fine.
Heretic
Re: Re: Re: Re: Atkins Diet
by bill7b, on 7/24/2003 4:13:16 PM
NEW!
The "official" upper limit for normal blood
glucose was 120 until two years ago. A lot of knowledgeable doctors were
using 110 as the guideline for a year or more before the official change.
It hasn't been 140 for a long time.
You are also incorrect about the method
used for diagnosing diabetes. It may be one means, but it certainly isn't
the standard.
Apparently, for you this may be theory
and stuff you can get from books. For diabetics having the right information
is the difference between life and death, sight and blindness, having limbs
or not, being fully functioning or not.
It bothers me that you are representing
something incorrect or at least outdated as being true and current, in
a way that could get people in a lot of trouble. It will bother me a lot
more if you are adamant in not recognizing that it is you who are out of
step with the official medical guidelines. It's not so bad being wrong
(I often am) or having an honest difference of opinion, it's being persistent
in the face of better information that's a problem.
Have a nice day.
Bill
Re: Re: Re: Re: Re: Atkins Diet
by Heretic, on 7/24/2003 8:36:02 PM
NEW!
Bill,
You are correct, my numbers may be somewhat
off, especially if I quote it from memory, I was trying to illustrate the
principle. Appologies.
You are also correct that your practical
experience with diabetes is worth more than mine (theoretical).
You are also correct that I do not adhere
to the officlal medicine.
However we are living in special times
when the official medical guidelines in nutrition and diabetes have shown
to be of very little practical value. They do not seem to work!
In this special case I take a liberty to
NOT to keep my mouth shut and to speak out about some alternatives that
MIGHT work whereas the mainstream medical procedures are PROVEN by decades
of use - and are GUARANTEED to keep you progressively more sick. If you
have heard of any diabetic getting better over years, following the mainstream
diabetic guidelines, please tell me, I would be very interested to know
of one such case. If it does exist.
The issue of maintaining certain glucose
level is more important and more tricky than people realize.
However, the optimal level is not necessary
the one just above fainting from hypoglycemia!
This is quite counter-intuitive - I need
to explain. The optimal level is such that it minimizes your insulin intake
while still keeping your glucose below the upper limit of, let's say 140mg/dl.
If you, for instance manage to keep it
in the range of for example 100-140mg/dl with for example 40 insulin units
per day - you are much better off than if you tried to maintain it by brute
force within 60-100 band at a cost of for example doubling your insulin
to 80 insulin units per day. The relation is non-linear because your liver
would produce extra glucose if glucose level falls too low.
Most important is to keep in mind that
not only high glucose level is a risk factor but HIGH insulin level is
risky as well! By keeping your insulin level reasonably low you may be
reducing yor risk of necrotic warts on your feet and hands, and other complications
- including arteriosclerosis and CVD, even if your glucose may be higher
than 110! As you can see, it is not as simple as just keeping your glucose
below 110.
Take care,
Heretic
P.S.
This is not only theoretical but based
on the experience of people who used to be diabetic , but no longer are.
